


By Dr. Neel Patel, MS ENT
Endoscopic ENT Surgeon, Ahmedabad
Summary
Otosclerosis is a progressive ear condition affecting thousands in Gujarat and across India, causing gradual hearing loss as abnormal bone growth immobilizes the tiny stapes bone in the middle ear. What many don’t realize is that this condition is completely reversible through advanced Laser Stapedotomy surgery. At Harsiddh ENT Clinic and Shaleen Hospital in Ahmedabad, Dr. Neel Patel combines cutting-edge laser technology with modern endoscopic techniques to restore hearing with unprecedented precision. This minimally invasive procedure boasts a 90-95% success rate, requires no external incisions, and allows most patients to return to normal activities within a week. Unlike traditional methods, the laser approach is contactless, bloodless, and accurate to the micron level, while the endoscopic visualization allows surgeons to see around corners inside the ear—something impossible with conventional microscopes. If you’re experiencing progressive hearing loss, constantly asking people to repeat themselves, or struggling with tinnitus, this article explains how modern otosclerosis treatment in Ahmedabad can restore your world of sound.
Introduction: When Silence Slowly Takes Over
Imagine sitting in a family gathering, watching everyone’s lips move but struggling to catch the words. You find yourself nodding along, pretending to understand, while internally feeling isolated from the very people you love. The television volume keeps creeping higher, earning you complaints from family members. Phone conversations become exercises in frustration as you repeatedly ask “What? Can you say that again?”
This is the daily reality for thousands of people living with otosclerosis—a condition that slowly but steadily steals the gift of hearing.
If you’ve noticed your hearing gradually declining, especially if you’re in your 20s, 30s, or 40s, and particularly if you’re a woman (otosclerosis affects women twice as often as men), you might be experiencing this condition. The good news? Unlike many forms of hearing loss, otosclerosis is completely reversible through surgery.
Welcome to the world of modern otosclerosis treatment in Ahmedabad, where advanced Laser Stapes Surgery—particularly when performed using state-of-the-art endoscopic techniques—is restoring hearing and transforming lives with remarkable success rates and minimal discomfort.
What is Otosclerosis? Understanding the Silent Thief of Hearing
The Medical Definition
Otosclerosis (from the Greek words “oto” meaning ear, and “sclerosis” meaning abnormal hardening) is a condition where abnormal bone growth occurs in the middle ear, specifically around the stapes bone—the smallest bone in the human body and a critical component of your hearing mechanism.
How Your Hearing Works (And What Goes Wrong)
To understand otosclerosis, let’s first understand how we hear:
- Sound waves enter your ear canal and hit your eardrum (tympanic membrane)
- The eardrum vibrates and transfers these vibrations to three tiny bones in your middle ear: the malleus (hammer), incus (anvil), and stapes (stirrup)
- The stapes bone acts like a piston, pushing against the oval window—the entrance to your inner ear
- This creates waves in the fluid of your inner ear (cochlea)
- These fluid waves stimulate hair cells that convert mechanical energy into electrical signals
- Your brain interprets these signals as sound
In otosclerosis, abnormal bone growth causes the stapes bone to become “frozen” or fixed to the surrounding bone structure. When the stapes can’t vibrate freely, sound can’t efficiently reach your inner ear. This is called conductive hearing loss—the sound is conducted poorly from the outer ear to the inner ear.
Think of it like trying to hear through a thick wall versus an open window. The sound is there, but it can’t reach you properly.
The Progression: How Otosclerosis Develops
Otosclerosis typically progresses through several stages:
Stage 1: Early/Active Otospongiosis
In the initial phase, there’s active remodeling of bone around the stapes footplate. The bone becomes “spongy” (hence the term otospongiosis) with increased blood vessel formation. At this stage, you might not notice any symptoms yet.
Stage 2: Sclerotic Phase
The spongy bone gradually hardens and becomes dense, progressively limiting stapes movement. This is when hearing loss becomes noticeable.
Stage 3: Advanced Fixation
Complete or near-complete fixation of the stapes footplate occurs, causing significant conductive hearing loss. In some cases, the abnormal bone growth can also affect the inner ear (cochlear otosclerosis), adding a sensorineural hearing loss component.
Common Symptoms: The Warning Signs
The symptoms of otosclerosis typically develop gradually and may include:
1. Progressive Hearing Loss
- Usually begins in one ear, though both ears are eventually affected in 70-80% of cases
- You may notice difficulty hearing low-pitched sounds and whispers
- Hearing often seems worse in quiet environments and paradoxically better in noisy places (paracusis of Willis phenomenon—background noise masks the hearing difficulty)
2. Tinnitus (Ringing in the Ears)
- Affects approximately 75% of otosclerosis patients
- Can range from mild ringing to loud roaring sounds
- May worsen as the condition progresses
- Often described as hissing, buzzing, or humming
3. Speaking Softly (Autophony)
- You may start speaking more quietly because your own voice sounds abnormally loud to you
- This happens because bone conduction (how you hear your own voice) remains normal while air conduction is reduced
4. Dizziness or Balance Problems
- Less common but can occur in 25-30% of cases
- Usually mild and intermittent
- More pronounced if the inner ear is involved (cochlear otosclerosis)
Who Gets Otosclerosis? Risk Factors and Prevalence
Demographics:
- Age of onset: Usually between 15-45 years, with peak incidence in the 20s and 30s
- Gender: Women are affected 2:1 compared to men
- Ethnicity: More common in Caucasians (approximately 1-2% prevalence), less common in Asian and African populations (0.1-1%)
- Geographic variation: In India, particularly in urban centers like Ahmedabad, Surat, and other parts of Gujarat, awareness and diagnosis are increasing with better access to specialized ENT care
Key Risk Factors:
- Genetics (Most Significant Factor)
- 50-60% of patients have a family history
- If one parent has otosclerosis, children have 25% chance of developing it
- If both parents are affected, the risk increases to 50%
- Multiple genes have been implicated, though inheritance pattern is complex (likely autosomal dominant with incomplete penetrance)
- Hormonal Factors
- Pregnancy often accelerates the condition (estrogen may stimulate bone remodeling)
- Some women first notice symptoms during or after pregnancy
- Hormonal contraceptives may influence progression
- Measles Virus
- Some research suggests a potential link between measles virus RNA and otosclerosis development
- This theory remains under investigation
- Stress Fractures
- Repeated minor trauma to the ear may trigger abnormal bone remodeling in susceptible individuals
- Autoimmune Factors
- Emerging research suggests possible autoimmune components in some cases
The Emotional and Social Impact
Beyond the medical statistics, otosclerosis profoundly affects quality of life:
- Social withdrawal: Difficulty following conversations leads to avoiding social gatherings
- Professional challenges: Meetings, phone calls, and workplace communication become stressful
- Relationship strain: Loved ones may feel you’re not listening or don’t care
- Mental health: Depression and anxiety are common among untreated patients
- Safety concerns: Inability to hear warning signals, traffic, or alarms
The isolation can be overwhelming. Many patients describe feeling like they’re watching life through a glass window—present but not fully participating.
The Modern Solution: Laser Stapes Surgery (Stapedotomy)
What is Stapedotomy?
Stapedotomy, also known as stapes surgery or laser stapes surgery, is the gold-standard surgical treatment for otosclerosis. It’s one of the most successful operations in all of medicine, with success rates consistently exceeding 90-95% in experienced hands.
The term “stapedotomy” specifically refers to creating a small hole (Greek: “tome” = to cut) in the stapes footplate, as opposed to “stapedectomy” which involves removing the entire footplate. Modern practice favors stapedotomy because it’s safer and produces excellent results.
The Surgical Concept: Replacing What’s Frozen
Since the stapes bone is frozen and cannot vibrate, the solution is elegant: remove or bypass the immobilized stapes and replace it with an artificial prosthesis (a tiny piston) that can vibrate freely.
The Basic Steps:
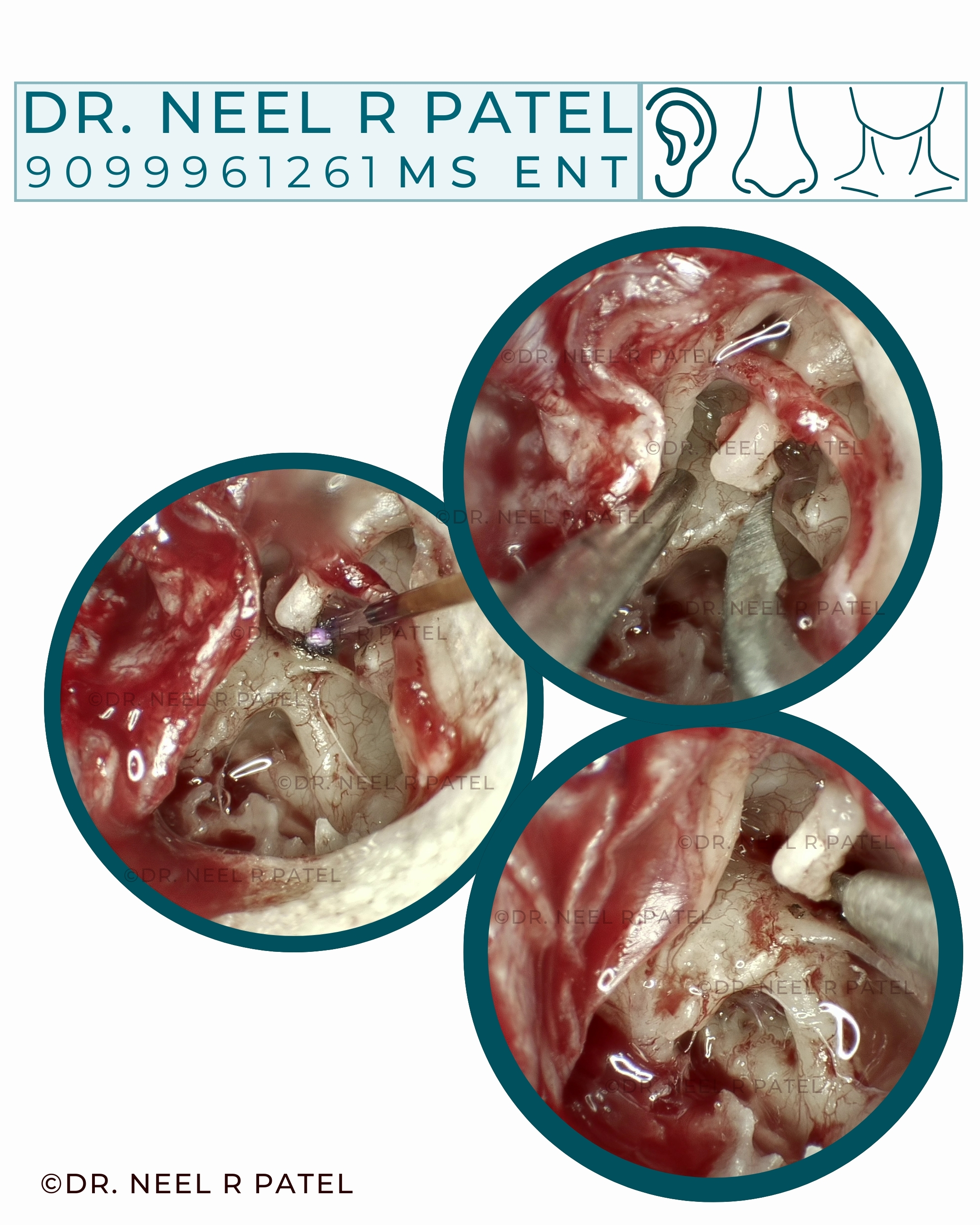
- Access: The surgeon works through your ear canal (no external cuts in most cases)
- Visualization: Using an endoscope or microscope, the surgeon carefully lifts the eardrum to expose the middle ear
- Removal: The superstructure (top part) of the stapes is carefully removed
- Creating an opening: A precise, tiny hole (0.6-0.8mm) is made in the stapes footplate
- Prosthesis placement: A small piston (usually made of Teflon, titanium, or platinum) is inserted through this hole
- Connection: The prosthesis is connected to the incus (the bone above the stapes), creating a new pathway for sound vibrations
- Closure: The eardrum is returned to its normal position and packing material is placed
The Laser Advantage: Why CO2 Laser Technology Transforms the Procedure
Traditional stapes surgery relied on manual drilling and mechanical instruments to create the opening in the footplate. While effective, this approach had limitations. Enter the laser—a game-changer in otologic surgery.
Key Advantages of Laser Stapedotomy:
1. Contactless Precision
The laser operates without physically touching the delicate inner ear structures. This dramatically reduces:
- Trauma to the inner ear
- Risk of displacement of footplate fragments
- Acoustic trauma from mechanical drilling
- Vibration-induced damage
2. Micron-Level Accuracy
CO2 lasers can create a perfectly round hole with precision measured in microns (thousandths of a millimeter). This level of accuracy is simply impossible with hand-held drills, no matter how skilled the surgeon.
3. Bloodless Field
The laser instantly cauterizes tiny blood vessels as it works, maintaining a clear, dry surgical field. This gives the surgeon:
- Better visualization of critical structures
- Reduced operative time
- Lower risk of complications
- More precise control throughout the procedure
4. Reduced Heat Injury
Modern CO2 lasers use ultra-short pulses (microseconds) that vaporize bone without heating surrounding tissues. The heat dissipates before it can damage sensitive inner ear structures.
5. Controlled Bone Removal
The laser removes bone in a controlled, layer-by-layer fashion. The surgeon can:
- Stop immediately if the footplate becomes mobile
- Avoid “plunging” through the footplate (a risk with mechanical drilling)
- Create the exact size hole needed for the prosthesis
6. Lower Risk of Perilymph Gusher
The controlled nature of laser drilling reduces the risk of sudden, forceful outflow of inner ear fluid (perilymph), which can occur with mechanical perforation.
The Clinical Evidence: What the Research Shows
Multiple studies have compared laser versus non-laser stapedotomy:
- Hearing improvement: Both achieve excellent results (90-95% success), but laser shows slightly better high-frequency hearing preservation
- Complication rates: Laser stapedotomy demonstrates lower rates of sensorineural hearing loss (0.3-0.5% vs 1-2% with mechanical)
- Vertigo: Postoperative dizziness tends to be less severe and shorter-lasting with laser
- Revision surgery: If needed years later, laser-created openings are easier to work with
Why Choose Endoscopic Surgery? The Latest Technique Revolution
While laser technology has transformed how we perform stapedotomy, endoscopic visualization has revolutionized how we see and access the surgical field. Dr. Neel Patel specializes in combining both technologies—endoscopic laser stapedotomy—offering patients the ultimate in precision and safety.
Understanding the Difference: Microscope vs. Endoscope
Traditional Microscopic Approach:
- Surgeon views the ear through a binocular operating microscope positioned outside the ear
- Provides straight-line, “line-of-sight” visualization only
- To see hidden areas, the surgeon must:
- Drill away healthy bone (canalplasty)
- Make wider incisions
- Manipulate delicate structures like the chorda tympani nerve
Modern Endoscopic Approach:
- A thin endoscope (3-4mm diameter) is inserted into the ear canal
- High-definition camera at the tip provides crystal-clear images on a large monitor
- Angled lenses (0°, 30°, 45°, or 70°) allow “seeing around corners”
- Surgeon can visualize hidden recesses without additional dissection
The Seven Critical Advantages of Endoscopic Stapes Surgery
1. Superior Visualization: Seeing the Invisible
The endoscope’s illumination comes from its tip, placed directly at the surgical site. Combined with angled lenses, this provides:
- Panoramic views: Wide-field visualization of the entire middle ear
- Around corners: Direct visualization of the oval window niche, even in difficult anatomies
- Hidden areas: Clear views of the facial recess, sinus tympani, and anterior epitympanum
- Better depth perception: Enhanced by HD imaging and magnification control
Research published in The European Archives of Oto-Rhino-Laryngology found that residents in training could identify the stapes footplate and oval window significantly better with endoscopes than microscopes, suggesting superior anatomical clarity.
2. Minimally Invasive Approach: No External Cuts
Most endoscopic stapedotomies can be performed entirely through the ear canal (transcanal approach):
- No postauricular (behind-the-ear) incision needed in most cases
- No endaural (in front of the ear) incision required
- No visible scars
- Reduced soft tissue trauma
- Faster recovery time
3. Preserved Anatomy: Protecting What Matters
Because the endoscope provides superior visualization without requiring a straight line of sight:
- Less bone removal: The bony external auditory canal (scutum) often doesn’t need drilling
- Chorda tympani nerve preservation: This taste nerve can be preserved more reliably (preserved in ~95% of endoscopic cases vs ~85-90% microscopic)
- Reduced manipulation: Less retraction and movement of delicate structures
4. Reduced Postoperative Pain and Faster Recovery
Clinical studies comparing endoscopic and microscopic ear surgery consistently show:
- Less pain: Patients report significantly lower pain scores after endoscopic procedures
- Shorter hospital stay: Most patients go home the same day
- Faster healing: Average healing time of 5-6 weeks compared to 7-8 weeks with open approaches
- Quicker return to work: Most patients return within 7-10 days
5. Challenging Anatomies Made Manageable
Some patients have anatomical variations that make microscopic surgery particularly difficult:
- Narrow ear canals
- Anterior bony overhang
- Low-lying tegmen (roof of middle ear)
- Prominent facial nerve
In these cases, the endoscope’s ability to see around corners makes surgery possible without extensive bone removal or alternative approaches.
6. Better Outcomes in Terms of Residual Disease
For patients requiring revision surgery or those with complex pathology, studies show:
- Lower rates of residual disease (5% vs 22.5% in some studies)
- Lower recurrence rates (7.5% vs 27.5%)
- Better preservation of existing reconstructions during second-look procedures
7. Educational Advantage: Better Training for Future Surgeons
The endoscope display on a high-definition monitor allows:
- The entire surgical team to see exactly what the surgeon sees
- Better understanding of anatomy for assistants and trainees
- Improved safety through team awareness
- Educational recordings (with patient consent) for continuous quality improvement
The Evidence: What Research Shows About Endoscopic Stapedotomy
Recent studies from leading international centers demonstrate:
- Success rates: Equivalent to microscopic surgery (90-95% achieve air-bone gap closure to <10 dB)
- Complication rates: Similar or lower than microscopic approach
- Patient satisfaction: Higher due to no external incision, less pain, and faster recovery
- Surgical time: After the learning curve, equivalent or faster than microscopic surgery
- Long-term outcomes: Durable hearing improvement maintained over years
A 2024 randomized controlled trial comparing endoscopic and microscopic stapedotomy in the same patients (one ear each method) found no difference in hearing outcomes but significantly higher patient preference for the endoscopic side due to reduced postoperative discomfort.
The Combination: Endoscopic + Laser = Optimal Results
When you combine endoscopic visualization with CO2 laser technology, you get:
- The precision and safety of laser bone removal
- The superior visualization and minimal invasiveness of endoscopy
- The ability to see exactly where the laser is working in real-time
- Reduced operative time compared to microscopic laser surgery
- Optimal outcomes with maximum safety
This is the approach Dr. Neel Patel has pioneered in Ahmedabad—bringing international best practices to Gujarat.
Understanding the Risks: An Honest Discussion About Complications
Every surgical procedure carries risks, and stapes surgery is no exception. However, it’s important to understand these risks in context. Modern laser stapedotomy with endoscopic visualization, performed by experienced surgeons, is one of the safest and most successful operations in all of medicine.
Let’s discuss complications honestly, transparently, and with proper perspective.
Overall Risk Profile
In experienced hands at high-volume centers:
- Success rate (significant hearing improvement): 90-95%
- No change in hearing: 3-5%
- Worsening of hearing (severe): 0.5-1%
- Total hearing loss: <0.5% (extremely rare)
Detailed Complication Analysis
Common and Expected (Not Really “Complications”)
1. Temporary Taste Disturbance (60-70% of patients)
What happens: The chorda tympani nerve, which carries taste sensation from the front two-thirds of your tongue, runs through the middle ear very close to where surgery is performed. It often must be gently moved aside during surgery.
Symptoms:
- Altered or metallic taste on the side of the tongue (same side as surgery)
- Most noticeable with salty or sweet foods
- Usually described as mild to moderate
Recovery:
- 95-96% of patients recover completely within 6-12 months
- Only 4-5% have persistent but mild taste changes
- The brain typically adapts even if complete recovery doesn’t occur
Patient perspective: “It was strange for a few weeks—coffee tasted a bit metallic. By three months, I barely noticed it, and by six months, it was completely normal.”
2. Immediate Postoperative Dizziness (50-60% of patients)
What happens: The inner ear’s balance system is temporarily disturbed during surgery when the stapes is removed and the prosthesis inserted.
Symptoms:
- Spinning sensation (vertigo) immediately after surgery
- Usually lasts a few hours to 2-3 days
- Mild unsteadiness or motion sensitivity for 1-2 weeks
Management:
- Anti-vertigo medications (given preventively)
- Rest for first 24-48 hours
- Gradual increase in activity
Recovery: 98% of patients have complete resolution within 1-2 weeks.
3. Temporary Hearing Fluctuation (30-40% of patients)
What happens: Fluid and blood in the middle ear immediately after surgery, combined with packing materials, temporarily affect hearing.
Timeline:
- First week: Hearing often worse than before surgery (muffled, like underwater)
- Weeks 2-4: Dramatic improvement as packing absorbs and inflammation resolves
- Weeks 4-12: Continued gradual improvement to final result
Patient experience: “My doctor warned me about this, so I wasn’t worried. By the second week when the packing dissolved, it was like someone turned the volume up on life!”
Uncommon Complications (1-5% of cases)
4. Prolonged Vertigo (2-3%)
Causes:
- Prosthesis slightly too long
- Small perilymph leak
- Inner ear inflammation
Symptoms: Dizziness persisting beyond 2 weeks
Management:
- Usually resolves with time and vestibular rehabilitation
- Rarely requires revision surgery (if prosthesis length is the issue)
5. Temporary High-Frequency Hearing Loss (3-5%)
What happens: Some patients experience a temporary dip in high-frequency hearing (sounds like “s,” “th,” “f”).
Timeline: Most recover within 6-9 months as inner ear inflammation resolves.
Note: This is different from permanent sensorineural hearing loss (see below).
6. Tympanic Membrane Perforation or Tear (1-2%)
What happens: Small tear in the eardrum during surgery or healing.
Management:
- Small tears often heal on their own with conservative treatment
- Larger tears may require patch or repair
Serious but Rare Complications (<1%)
7. Permanent Sensorineural Hearing Loss (0.3-0.5% with laser)
What happens: Direct injury to the inner ear’s delicate hair cells or structures.
Causes:
- Excessive manipulation of the stapes
- Bone fragments falling into the vestibule
- Prosthesis trauma to inner ear
- Acoustic trauma from drilling (much less common with laser)
- Perilymph leak
Severity: Can range from mild high-frequency loss to severe/profound hearing loss.
Impact: If severe, hearing aid may be needed; if profound, hearing aid may not help (consideration for cochlear implant in rare cases).
Risk reduction with laser + endoscopy:
- Laser eliminates mechanical vibration trauma
- Endoscope provides better visualization to avoid inner ear trauma
- Combined approach reduces risk to approximately 0.3% (3 in 1,000 cases)
8. Complete Hearing Loss (Anacusis) (<0.5%)
What happens: Total loss of hearing in the operated ear.
Causes:
- Severe inner ear injury
- Infection (extremely rare with modern sterile techniques)
- Labyrinthitis (inner ear inflammation)
- Unknown causes in some cases
Impact: This is the most devastating complication. The ear would not benefit from conventional hearing aids. Bone-anchored hearing aids or cochlear implants would be considered.
Prevention:
- Operating only on the worse-hearing ear first
- Waiting 6-12 months before operating on the second ear
- Thorough preoperative evaluation to identify high-risk patients
- Meticulous surgical technique
9. Facial Nerve Paralysis (<0.1%—extremely rare)
What happens: The facial nerve runs very close to the surgical field. In rare cases with anomalous nerve anatomy, it can be injured.
Types:
- Immediate (recognized during surgery): Usually from heat or direct trauma
- Delayed (days after surgery): Usually from inflammation or viral reactivation
Management:
- Immediate exploration if recognized
- High-dose steroids
- Eye protection (if eyelid affected)
- Most delayed cases recover fully
Prevention:
- Careful anatomical identification
- Facial nerve monitoring (in some centers)
- Cautious use of laser near the nerve
- Endoscopic visualization of nerve course
10. Perilymphatic Fistula (0.5-1%)
What happens: Abnormal connection between the inner ear and middle ear allows inner ear fluid (perilymph) to leak out.
Symptoms:
- Fluctuating hearing loss
- Positional vertigo
- Pressure sensitivity (symptoms with sneezing, straining, flying)
Management:
- Conservative (bed rest, avoid straining) initially
- Surgical repair if persistent
Very Rare and Unusual Complications
11. Reparative Granuloma (0.5-1%)
What happens: Inflammatory tissue forms around the prosthesis, usually in the first 2 weeks.
Symptoms:
- Sudden worsening hearing
- Severe vertigo
- Ear pain
- Violaceous (purplish) mass visible behind eardrum
Management:
- Urgent surgical removal
- High-dose corticosteroids
- Prosthesis replacement
Prognosis: If treated promptly, hearing can often be preserved. Delay can lead to permanent hearing loss.
12. Prosthesis Problems (Long-term, 1-2% over 10-20 years)
Types:
- Displacement/migration
- Extrusion
- Loosening of connection to incus
- Bone regrowth closing the opening (neootosclerosis)
Timing: Usually years after initial surgery.
Symptoms: Gradual return of hearing loss.
Management: Revision surgery, usually successful.
Putting Risks in Perspective: Comparison with Daily Life Risks
It’s human nature to focus on surgical risks while ignoring the risks we accept daily without thought. Let’s put stapes surgery risks in context:
| Activity/Scenario | Risk of Serious Injury or Death | Comparison to Stapedotomy |
|---|---|---|
| Laser Stapedotomy – Complete Hearing Loss | 1 in 200-400 (0.25-0.5%) | Baseline risk |
| Driving a car in India (annual risk of serious accident) | ~1 in 100 (1%) | 2-4x higher than surgery |
| Crossing a busy road in Ahmedabad (lifetime risk) | Significantly higher | Much higher than surgery |
| Airplane travel (per flight, serious incident) | 1 in 11 million | Much lower than surgery |
| General anesthesia (serious complication) | 1 in 10,000-20,000 | Similar to surgery |
| Taking NSAIDs regularly (serious GI bleed annually) | 1 in 1,000 | lower than surgery |
| Untreated otosclerosis (progressive to severe hearing loss) | Nearly 100% over 10-20 years | Surgery prevents this |
What this means:
- The risk of serious complication from stapedotomy (0.5-1%) is comparable to or lower than risks we routinely accept in daily life
- The risk of progressive hearing loss if you do nothing approaches 100%
- For most patients, the risk-benefit ratio heavily favors surgery
Special Considerations
If you have otosclerosis in both ears:
- The worse-hearing ear is always operated on first
- This ensures you always have your better ear for hearing
- The second ear (if needed) is operated on 6-12 months later
- Even in the rare event of complete hearing loss, you have the unoperated ear
If you only have otosclerosis in one ear:
- The risk-benefit discussion is more nuanced
- Factors to consider:
- Severity of hearing loss
- Impact on quality of life
- Occupation and communication needs
- Patient’s risk tolerance
- Surgeon’s experience and success rate
Age considerations:
- Stapes surgery is safe from adolescence through elderly years
- Older patients (>40 years) may have slightly higher rates of temporary high-frequency hearing loss, but this typically recovers
- Age alone is rarely a contraindication
Questions to Ask Your Surgeon
Before deciding on surgery, have an honest conversation with your surgeon:
- “What is your personal success rate with this operation?”
- “How many stapes surgeries do you perform per year?”
- “What is your complication rate?”
- “Have you had any cases of complete hearing loss, and if so, what happened?”
- “Do you use laser and endoscopic techniques?”
- “What happens if my hearing doesn’t improve?”
- “What is your plan if complications occur?”
Dr. Neel Patel’s Approach: At Harsiddh ENT Clinic and Shaleen Hospital, Dr. Patel maintains detailed records of all surgical outcomes. His practice philosophy emphasizes:
- Thorough preoperative evaluation and patient selection
- Use of the latest technology (laser + endoscopy) for maximum safety
- Transparent discussion of personal outcomes and complications
- Comprehensive postoperative care and long-term follow-up
- Immediate availability for concerns or complications
The Patient Journey: What to Expect
Preoperative Evaluation
Initial Consultation:
- Detailed medical history
- Discussion of symptoms and impact on life
- Examination of ears with endoscope
- Basic hearing test (tuning fork tests)
Comprehensive Audiological Testing:
- Pure Tone Audiometry (PTA): Measures hearing at different frequencies
- Speech Audiometry: Assesses speech understanding
- Tympanometry: Evaluates eardrum movement
- Acoustic Reflex Testing: Checks middle ear function
- Bone Conduction Testing: Differentiates conductive vs sensorineural hearing loss
Expected findings in otosclerosis:
- Conductive hearing loss (air-bone gap of 30-60 dB typical)
- Normal or near-normal bone conduction (unless cochlear otosclerosis)
- Classic “Carhart notch” at 2000 Hz on bone conduction
- Absent acoustic reflexes (stapedial reflex)
Imaging (if needed):
- High-resolution CT scan of temporal bones
- Confirms diagnosis
- Rules out other conditions
- Identifies anatomical variations
- Not always necessary in straightforward cases
Discussion and Consent:
- Dr. Patel explains the procedure in detail
- Discussion of risks, benefits, and alternatives
- Realistic expectations about outcomes
- Questions answered thoroughly
- Written informed consent
The Day of Surgery
Preparation:
- Fasting (usually 6-8 hours before surgery)
- Arrival 1-2 hours before scheduled time
- Pre-anesthetic evaluation
- IV line placement
Anesthesia Options:
- General Anesthesia (most common at Shaleen Hospital/Harsiddh ENT Clinic)
- You’re completely asleep
- No awareness or memory of surgery
- Better patient comfort
- Allows for completely motionless field
- Local Anesthesia with Sedation (selected cases)
- Numbing medicine in the ear
- Sedative medication for relaxation
- Patient is drowsy but responsive
- Surgeon can get feedback about hearing during surgery
Surgical Duration:
- Typical duration: 60-90 minutes
- May vary based on anatomy and findings
Immediate Post-Surgery:
- Recovery room for 2-4 hours
- Monitoring for dizziness, nausea
- Anti-vertigo medications given preventively
- Most patients go home the same day
Recovery Timeline
Day 1-3: Initial Recovery
- Expect: Mild to moderate dizziness, fullness in ear, muffled hearing
- Do: Rest at home, take prescribed medications, keep ear dry
- Don’t: Blow nose, bend over, lift heavy objects, get water in ear
Week 1: Early Healing
- First follow-up visit (usually day 5-7)
- Cotton ball removed from ear canal
- Hearing still muffled (packing still in place)
- Gradual improvement in balance
- Expect: Some blood-tinged drainage on cotton ball is normal
Weeks 2-4: Dramatic Improvement
- Packing material starts dissolving (usually gelfoam)
- Sudden improvement in hearing often noticed
- Can usually return to work (desk jobs)
- Avoid: Heavy lifting, straining, contact sports
Weeks 4-6: Near-Complete Healing
- Second follow-up with hearing test
- Assessment of surgical success
- Most restrictions lifted
- Can resume most normal activities
Months 3-6: Final Results
- Continued subtle improvement possible
- Final hearing test to document outcome
- Full release to all activities including swimming, flying
Postoperative Precautions
For 2 Weeks:
- No nose blowing (sneeze with mouth open)
- No straining or heavy lifting (>10 kg)
- Keep ear completely dry (cotton ball with petroleum jelly while bathing)
- No swimming or air travel
For 4 Weeks:
- Avoid contact sports
- Avoid very loud noise exposure
- Gradual return to exercise
Long-term:
- Some surgeons recommend avoiding scuba diving permanently
- Inform future doctors that you’ve had stapes surgery
- Carry surgery documentation when flying (for security purposes)
Success Rates and Expected Outcomes
Hearing Improvement:
- 90-95% of patients achieve successful hearing improvement
- “Success” defined as closing the air-bone gap to ≤10 dB
- 70-80% achieve normal or near-normal hearing
- Results are typically durable for 10-20+ years
Quality of Life:
- Return to comfortable conversation without asking people to repeat
- Able to use telephone easily
- Reduced TV volume
- Improved confidence in social situations
- Reduced tinnitus in 60-70% of cases
- Enhanced professional performance
Long-term Durability:
- 85-90% maintain excellent hearing at 10 years
- 75-80% maintain excellent hearing at 20 years
- If hearing declines years later, revision surgery is often successful
Meet the Expert: Dr. Neel Patel – Pioneer of Advanced Endoscopic Ear Surgery in Ahmedabad
Qualifications and Training
Dr. Neel Patel, MS ENT
Fellowship in Endoscopic ENT Surgeries
Specialist in Micro-Ear and Advanced Otologic Surgery
Dr. Neel Patel brings a unique combination of advanced training, cutting-edge technology, and patient-centered care to the field of otology in Ahmedabad and Gujarat. His journey represents the new generation of ENT surgeons who combine traditional surgical excellence with the latest minimally invasive techniques.
Education and Credentials:
- MS ENT (Master of Surgery in Ear, Nose, and Throat)
- Fellowship in Endoscopic ENT Surgeries from Talegaon, Maharashtra
- Advanced training in endoscopic sinus surgery
- Specialized endoscopic ear surgery techniques
- Endoscopic skull base surgery
- 5+ Years of Focused Experience in micro-ear and endoscopic surgeries
- Regular participation in national and international ENT conferences
- Multiple publications in peer-reviewed ENT journals
Professional Memberships:
- Association of Otolaryngologists of India (AOI), Ahmedabad
- Active participant in regional ENT education and advancement
- Society of Endoscopic Otolaryngologists (SEO)
- Membership in this specialized society demonstrates commitment to staying at the forefront of endoscopic ENT techniques
- Regular continuing medical education and training in latest surgical techniques
Surgical Philosophy: Combining Innovation with Safety
Dr. Patel’s approach to stapes surgery and otology represents the intersection of three critical elements:
1. Advanced Technology
- CO2 laser systems for precision and safety
- High-definition endoscopic visualization
- Latest prosthesis designs and materials
- State-of-the-art audiological testing equipment
2. Evidence-Based Practice
- Techniques based on latest international research
- Outcomes tracking and quality improvement
- Adoption of best practices from leading global centers
- Commitment to continuous learning
3. Patient-Centered Care
- Thorough explanation of diagnosis and treatment options
- Honest discussion of risks and benefits
- Individualized treatment plans
- Comprehensive pre- and postoperative support
- Long-term follow-up and relationship building
Why Dr. Patel’s Approach Stands Out in Gujarat
Specialized Focus: Unlike general ENT surgeons who perform a wide variety of procedures, Dr. Patel has dedicated his practice to advanced ear surgery, particularly:
- Otosclerosis and stapes surgery
- Chronic ear disease and tympanoplasty
- Cholesteatoma surgery
- Ossiculoplasty (middle ear reconstruction)
- Cochlear implant evaluations
This focused expertise translates to:
- Higher surgical volumes leading to better outcomes
- Refined technique and problem-solving abilities
- Up-to-date knowledge of latest advances
- Better management of complications (rare though they are)
Technological Leadership: Dr. Patel was among the first in Ahmedabad to adopt:
- Completely endoscopic ear surgery (without microscope)
- Laser stapedotomy as standard practice
- High-definition documentation for quality review
- Advanced audiological protocols
Educational Commitment: Beyond patient care, Dr. Patel is committed to advancing ENT surgery in Gujarat through:
- Training residents and fellows in endoscopic techniques
- Presentations at regional and national conferences
- Publications sharing surgical outcomes and innovations
- Community education about ear diseases
Patient Testimonials: Real Stories, Real Results
[Video Testimonial Available]
Watch a recent patient’s journey: https://youtube.com/shorts/ameYxSE6J9o?si=bHNDjvgSShKHJEh5
“I had been losing my hearing for three years. People thought I was ignoring them, but I just couldn’t hear. Dr. Patel explained everything so clearly, and I felt confident. The surgery was on Friday, and by the following week, I was back at work. Now, one month later, my hearing is completely normal. I wish I had done this sooner!”
— Patient testimonial (name withheld for privacy)
Research and Publications
Dr. Patel has contributed to advancing the field through research in:
- Outcomes of endoscopic versus microscopic ear surgery
- Hearing preservation techniques in stapedotomy
- Management of complications in otosclerosis surgery
- Endoscopic approaches to cholesteatoma
His publications in national and international ENT journals demonstrate his commitment to evidence-based practice and sharing knowledge with the broader medical community.
World-Class Facilities: Where You’ll Receive Care
Dr. Neel Patel operates from two state-of-the-art facilities in Ahmedabad, each offering comprehensive ear care with the latest technology and a patient-first approach.
Shaleen Hospital Multispecialty
Advanced Infrastructure: Shaleen Hospital represents the pinnacle of modern ENT care in Ahmedabad, with:
- Fully equipped operation theaters with laminar flow
- High-definition endoscopic towers
- laser systems
- Comprehensive audiological testing suite
- ICU facilities for complex cases
- General ward and private rooms
- Post-anesthesia care unit (PACU)
- 24/7 emergency support
Technology and Equipment:
- Latest generation surgical microscopes
- 4K endoscopic equipment
- Advanced anesthesia monitoring systems
- Digital documentation and archiving
Patient Amenities:
- Cashless facility with all major insurance providers
- Comfortable waiting areas for families
- Patient counseling rooms
- Pharmacy on-site
- Laboratory services
Location and Timing:
Shaleen Hospital Multispecialty
4th Floor, Shaleen Plaza
Sola Gam Road, Nr Mangaldeep Capital
Ahmedabad, Gujarat 380060
Timings: Monday – Saturday, 10:00 AM – 1:00 PM
Contact:
📧 doctor.neel.ent@gmail.com
📞 +91-9099961261 (Dr. Patel)
📞 +91-9512039041 (Appointments/Emergency)
Harsiddh ENT Clinic
Mission-Driven Care: Harsiddh ENT Clinic is run by a medical trust with a clear mission: providing world-class ENT care at affordable prices to all sections of society. This commitment to accessibility without compromising quality makes advanced ear surgery available to a wider population in Gujarat.
Facilities:
- Modern outpatient consultation rooms
- Complete audiological testing suite
- Endoscopic examination and minor procedure rooms
- Comfortable waiting areas
- Counseling and education areas
Philosophy:
- High-quality care at affordable rates
- Focus on patient education and shared decision-making
- Personalized attention with adequate consultation time
- Strong emphasis on preventive care and early intervention
Location and Timing:
Harsiddh ENT Clinic
201B, Shivam Complex
Bhuyangdev Cross Road
Ahmedabad, Gujarat 380061
Timings:
- Monday – Friday: 5:00 PM – 8:00 PM
- Saturday: 4:00 PM – 7:00 PM (By Appointments Only)
Contact:
📧 doctor.neel.ent@gmail.com
📞 +91-9099961261
📞 +91-79-27496329
Frequently Asked Questions
Q: How long will my hearing improvement last?
A: Stapes surgery provides durable results. 85-90% of patients maintain excellent hearing at 10 years, and 75-80% at 20 years. If hearing gradually declines years later (uncommon), revision surgery is usually successful.
Q: Will I need surgery on both ears?
A: About 70-80% of otosclerosis patients eventually develop the condition in both ears. However, we always operate on one ear at a time, waiting 6-12 months between surgeries. Many patients find that improving one ear is sufficient for their needs.
Q: Can I fly after stapes surgery?
A: You should avoid flying for 4-6 weeks after surgery. After that, flying is generally safe. Some surgeons recommend avoiding frequent flying or being cautious with pressure changes, but most patients can fly normally.
Q: Will the surgery affect my balance permanently?
A: Temporary dizziness is common for a few days after surgery, but permanent balance problems are very rare (<1%). The inner ear’s balance system typically adapts quickly.
Q: What if I don’t have surgery? Can I just use a hearing aid?
A: Hearing aids can help with otosclerosis and are a reasonable option if you prefer to avoid surgery. However:
- Otosclerosis is progressive—it will continue to worsen
- Hearing aids don’t address the underlying problem
- Surgery offers a permanent solution in most cases
- Many patients find hearing aids uncomfortable or insufficient
- Surgery is generally cost-effective compared to lifelong hearing aid use
Q: How soon will I notice improvement in my hearing?
A: This varies. Some patients notice improvement immediately after surgery (while still on the operating table with local anesthesia). However, most patients’ hearing is worse initially due to packing and fluid, then dramatically improves around weeks 2-4 as these resolve. Final hearing results are assessed at 3-6 months.
Q: Is stapes surgery covered by insurance?
A: Most health insurance policies in India cover stapes surgery as it’s a medically necessary procedure. At Shaleen Hospital, we offer cashless facility with all major insurance providers. The team can help verify your coverage and handle insurance paperwork.
Q: What is the cost of laser stapes surgery in Ahmedabad?
A: Costs vary based on the facility, type of anesthesia, length of hospital stay, and specific techniques used. At Harsiddh ENT Clinic (run by a medical trust), care is provided at highly affordable rates. At Shaleen Hospital, comprehensive packages are available. Please contact the clinics directly for detailed cost information and insurance options.
Q: Can children have stapes surgery?
A: Stapes surgery is generally performed on patients after skeletal maturity (late teens onward). However, in rare cases of juvenile otosclerosis with severe hearing loss affecting education, surgery may be considered earlier. Each case is evaluated individually.
Q: What happens if the surgery doesn’t work?
A: If hearing doesn’t improve adequately:
- First, we wait 6 months as late improvements can occur
- We evaluate with detailed testing to understand why
- Revision surgery is often successful (success rate ~85%)
- Hearing aids remain an option
- In rare cases of total hearing loss, bone-anchored hearing aids or cochlear implants can be considered
Q: Can I exercise after stapes surgery?
A: Light walking can begin immediately. More strenuous exercise should be avoided for 4 weeks. Contact sports should be avoided for 6-8 weeks. Swimming should wait until cleared by your surgeon (usually 6-8 weeks).
Alternative and Complementary Treatments: What Else Is Available?
Hearing Aids
Who they’re for:
- Patients who prefer not to have surgery
- Those with medical contraindications to surgery
- Patients with cochlear otosclerosis (inner ear involvement)
- As a temporary measure before surgery
- If surgery doesn’t achieve full correction
Advantages:
- Non-invasive
- Immediately reversible
- No surgical risks
- Can be tried before deciding on surgery
Disadvantages:
- Don’t address the underlying problem
- Ongoing cost (devices need replacement every 5-7 years)
- Require maintenance and batteries
- Can be uncomfortable
- Less effective for severe conductive hearing loss
- Stigma for some patients
- Otosclerosis progresses despite hearing aid use
Sodium Fluoride Treatment
Theory: Sodium fluoride may slow the progression of otosclerosis by stabilizing bone metabolism.
Reality:
- Evidence is mixed and controversial
- May help in very early, active disease (otospongiosis phase)
- Does NOT reverse existing hearing loss
- Does NOT eliminate the need for surgery in most cases
- Side effects: Joint pain, stomach upset
- Not commonly prescribed today
Current role: Very limited; occasionally considered for bilateral disease when surgery is risky.
Observation (Watchful Waiting)
Appropriate for:
- Very mild hearing loss not affecting quality of life
- Only one ear affected with the other ear normal
- Medical conditions making surgery risky
- Patient preference
What it involves:
- Regular hearing tests (every 6-12 months)
- Monitoring for progression
- Re-evaluation of treatment options as disease progresses
Important to know: Otosclerosis almost always progresses. Waiting typically means operating at a more advanced stage later.
Bone-Anchored Hearing Aids (BAHA)
What they are: Surgically implanted devices that transmit sound through bone conduction, bypassing the middle ear entirely.
When considered:
- Failed stapes surgery with total hearing loss
- Congenital absence of the ear canal
- Chronic ear infections preventing conventional hearing aids
- Poor stapes surgery candidate for other reasons
Not a first-line treatment for otosclerosis unless special circumstances exist.
Understanding Your Audiogram: Reading Your Hearing Test Results
When you visit Dr. Patel, you’ll receive a comprehensive hearing evaluation. Understanding your audiogram helps you participate in treatment decisions.
Key Components of an Audiogram
Pure Tone Audiometry:
- X-axis: Frequency (pitch) from 250 Hz to 8000 Hz
- Y-axis: Intensity (loudness) from 0 dB (normal) to 120 dB (very loud)
- O symbols: Air conduction (right ear, sound through headphones)
- X symbols: Air conduction (left ear)
- < and > symbols: Bone conduction (sound transmitted through skull bone)
What Otosclerosis Looks Like:
- Air conduction line (O and X) shows hearing loss (drops below 20 dB)
- Bone conduction line (< and >) remains near normal
- Air-Bone Gap: The space between these lines is the hallmark of conductive hearing loss
- In otosclerosis, this gap is typically 30-60 dB
- Often shows “Carhart notch” at 2000 Hz on bone conduction (artifact of stapes fixation)
After Successful Surgery:
- Air conduction improves dramatically
- Air-bone gap closes to <10 dB
- Overall hearing approaches normal levels
Speech Audiometry
Speech Reception Threshold (SRT):
- Softest level at which you can repeat 50% of words
- Should match your pure tone average
- In otosclerosis, SRT is elevated but speech discrimination remains excellent
Speech Discrimination Score (SDS):
- Percentage of words correctly repeated at comfortable loudness
- Otosclerosis patients typically score 90-100% (excellent discrimination)
- This good discrimination is why surgery works so well
- If SDS is poor (<70%), suspect inner ear (cochlear) involvement
Tympanometry
What it measures: Eardrum mobility and middle ear pressure
Normal: Peak compliance around 0 daPa pressure, indicating normal eardrum movement
In Otosclerosis: “Type As” pattern—shallow or flat curve indicating reduced stapes mobility
Special Tests
Acoustic Reflex Testing:
- Measures stapedius muscle contraction in response to loud sound
- In otosclerosis: Reflexes are absent or elevated
- Helps confirm stapes fixation
CT Scan of Temporal Bones (when needed):
- Shows otosclerotic bone as “ground glass” opacity around oval window
- Rules out other causes of conductive hearing loss
- Identifies anatomical variants that affect surgery planning
- Not always necessary in straightforward cases
Living with One Operated Ear: What to Expect
Binaural vs. Monaural Hearing
Binaural (both ears): Our brains are designed to use both ears together for:
- Localizing where sounds come from
- Hearing in noisy environments
- Depth perception of sound
- Balance and spatial orientation
After operating on one ear:
- Dramatic improvement in overall hearing ability
- Better performance in most listening situations
- Some continuing challenges:
- Sound localization remains imperfect
- Very noisy environments may still be challenging
- Most patients are thrilled with improvement and don’t proceed to second ear surgery
If both ears need surgery:
- We always wait 6-12 months between surgeries
- This ensures complete healing and hearing stabilization
- You always have one ear that hasn’t been operated on (safety)
- Many patients choose to operate on the second ear for optimal hearing

Leave a Reply